There is no single test sufficient to diagnose MS (Polman et al. 2011, p. 121). Instead, confirming a diagnosis of MS requires multiple clinical and paraclinical studies. These studies are used to determine if a person meets the long-established criteria for a diagnosis of MS, and to rule out other possible causes of whatever symptoms the person is experiencing.
The table below shows the various possibilities to conclude a MS diagnosis (Polman et al. 2005, p. 844-845). Explanations of these tests are below.

What is an attack?
An attack is defined by patient-reported symptoms or objectively observed signs typical of an acute inflammatory demyelinating event in the CNS (Polman et al. 2011, p. 293). Examples of these types of symptoms vary and commonly include sensory disturbances, fatigue and/or motor impairment (Nickerson & Marrie, 2013, p. 2). An attack can either be current or historical, with duration of at least 24 hours; however they must not present with fever or infection (Polman et al. 2011, 293).
What is Magnetic Resonance Imaging (MRI)?
 Image received from: Costello, K & Harris, C. (2006). An Overview of Multiple Sclerosis: Diagnosis and Management Strategies. Retrieved from: http://www.medscape.com/viewarticle/527706_5
Image received from: Costello, K & Harris, C. (2006). An Overview of Multiple Sclerosis: Diagnosis and Management Strategies. Retrieved from: http://www.medscape.com/viewarticle/527706_5
A MRI is a medical imaging technique that shows areas of damaged tissue (lesions). There are lesions that are specific to MS patients (Polman et al. 2011, p. 294):
- Gadolinium-enhancing lesion or T2 hyperintense lesion (if no gadolinium enhancing lesion)
- Infratentorial lesion
- Juxtacortical lesion
- Periventricular lesions
- Spinal Cord
WHAT IS CEREBROSPINAL FLUID (CSF)?
|
CSF is obtained through a lumbar puncture. A lumbar puncture is when a needle is inserted at the base of the spine and CSF is collected to be analyzed (National Multiple Sclerosis Society, 2016). The CSF then undergoes isoelectric focusing technique. This is an electrophoretic technique that separates proteins based on their isoelectric point.
Compared to normal CSF, there are increased (at least 2 or more) oligoclonal IgG bands in MS CSF (Polman et al. 2011, p. 294). The increased values of IgG reflects the underlying autoimmune activation. |
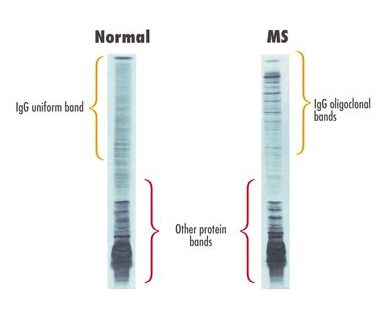
Image received from: Multiple Sclerosis Trust (2013). Lumbar Puncture. Retrieved from: https://www.mstrust.org.uk/a-z/lumbar-puncture
|
What is a Visual Evoked Potential (VEP) Test?
Patients who report visual disturbance may require a VEP test. This test corroborates the attacks that patients experience. This test measures the electrical activity (speed of nerve impulse conduction) of the brain in response to a visual stimulus (National Multiple Sclerosis Society, 2016). A person undergoing this test will have wires placed on their scalp overlying the areas of the brain that are being stimulated (National Multiple Sclerosis Society, 2016). The patient will watch a video, and the wires will record the responses of the person's brain.
Compared to normal VEP, it is delayed in MS. This is because nerve impulse conduction is slowed in MS related to the myelin damage, and VEP’s can record this slowing. This phenomenon is shown by Figure A.
In Figure B, it shows a VEP from someone who has early signs of MS. One nerve usually has normal nerve eye ranges, while the other is slowed (Creel, 2015). As you can see the right eye is normal, and the left eye is slowed. Patients with MS usually develop optic neuritis later in the other nerve, in this case the left nerve. As a patient's MS progresses, their VEPs develop in the other eye and eventually become much slower eventually attenuating in amplitude as demyelination increases (Creel, 2015).
Compared to normal VEP, it is delayed in MS. This is because nerve impulse conduction is slowed in MS related to the myelin damage, and VEP’s can record this slowing. This phenomenon is shown by Figure A.
In Figure B, it shows a VEP from someone who has early signs of MS. One nerve usually has normal nerve eye ranges, while the other is slowed (Creel, 2015). As you can see the right eye is normal, and the left eye is slowed. Patients with MS usually develop optic neuritis later in the other nerve, in this case the left nerve. As a patient's MS progresses, their VEPs develop in the other eye and eventually become much slower eventually attenuating in amplitude as demyelination increases (Creel, 2015).

Figure A: Image received from: Rose, J. (2016). Lectures: Laboratory Findings. Multiple Sclerosis. Retrieved from: http://library.med.utah.edu/kw/ms/mml/ms_vep.html
|

Figure B: Image received from: Creel, D. (2015).
Visually Evoked Potentials by Donnell J. Creel. Webvision. Retrieved from: http://webvision.med.utah.edu/book/electrophysiology/visually-evoked-potentials/
|
