Neurological assessment
RATIONALE: A neurological assessment is crucial to perform on patients with MS because MS is an inflammatory demyelinating disease of the CNS. A neurological assessment would therefore help monitor the effects of the MS on a patient's neurological status
(1) Test the Cranial Nerves
The table below shows how to conduct a cranial nerve assessment and the findings to expect with a patient who does not have MS. In patients with MS, the following could result.
(1) Test the Cranial Nerves
The table below shows how to conduct a cranial nerve assessment and the findings to expect with a patient who does not have MS. In patients with MS, the following could result.
- Cranial Nerve 1 (Olfactory)
- Instructions: Two different scents such as clove, vanilla or coffee. Have patient close eyes and close one nostril, then identify scent (Jarvis, 2014).
- Typical: Can identify smell (Jarvis, 2014).
- MS: Changes in smell can occur in MS (Devere, 2012)
- Cranial Nerve 2 (Optic)
- Instructions: Snellen chart or available print version and two index cards. Have patient identify writing or symbols. Assess peripheral vision by facing patient nose to nose 12 inches away. Have patient cover one eye with index card and you cover mirror image of eye (patient right eye, your left eye). Extend arm and have patient note when he or she sees fingers moving. Assess upper, middle and lower range of inner and outer aspect of eye. you should see finger movement at about the same time as the patient. If you (the examiner) have poor peripheral vision you will not be able to do the examination. (Jarvis, 2014)
- Typical: Comfortably and accurately reads or identifies small figures. Peirpheral vision intact (Jarvis, 2014).
- MS: Changes in Vision
- Double vision (diplopia) may hinder ability to read (Apatoff, 2014)
- Optic Neuritis: inflammation of the optic nerve. Symptoms include pain behind the eye (Apatoff, 2014)
- Cranial Nerve 3 (Oculomotor)
- Instructions: Hold penlight 12 inches from the patient's eyes. Next, have patient look at distant object then bring object close to patient eyes. Assess 6 cardinal positions of gaze
- Typical: Pupils constrict equally in response to light. Eyes are accommodating with convergence and constriction of pupils. Equal extraocular movement (Jarvis, 2014)
- MS: Nystagmus is possible and convergence should be intact (Apatoff, 2014).
- Cranial Nerve 4 (Trochlear)
- Instructions: Assess 6 cardinal positions of gaze.
- Typical: Eye movement is smooth towards the nose (Jarvis, 2014).
- MS: Nystagmus is possible, movements would not be smooth (Apatoff, 2014)
- Cranial Nerve 5 (Trigeminal)
- Instructions: Use a cotton ball and a dull end of an object such as a pen. Test sensation of the face. Have patient close eyes and identify when he or she feels touch. Wisp cotton ball against the cornea. Have the patient open their jaw against resistance (Jarvis, 2014).
- Typical: Conreal reflex intact. Sensation intact on forehead, jaw and cheek. Adequate jaw strength (Jarvis, 2014).
- MS: Intermittent unilateral facial numbness or pain (Apatoff, 2014). Decreased or unequal sensation (Jarvis, 2014).
- Cranial Nerve 6 (Abducens)
- Instructions: Assess 6 cardinal positions of gaze.
- Typical: Eye movement is smooth away from nose. A slight nystagmus at extreme lateral gaze is normal (Jarvis, 2014).
- MS: Nystagmus is possible in MS (Apatoff, 2014).
- Cranial Nerve 7 (Facial)
- Instructions: Ask patient to smile, frown or puff out cheeks (Jarvis, 2014).
- Typical: Equal facial expressions (Jarvis, 2014).
- MS: Facial palsy - drooping of face in MS (Apatoff, 2014).
- Cranial Nerve 8 (Acoustic)
- Instructions: Whisper next to patient ear but not in patient view to prevent lip reading (Jarvis, 2014).
- Typical: Able to understand whisper (Jarvis, 2014).
- MS: Hearing loss is possible (Apatoff, 2014).
- Cranial Nerve 9 (Glossopharyngeal) and Cranial Nerve 10 (Vagus)
- Instructions: Have patient say "ahh" using a tongue depressor. Test gag reflex (Jarvis, 2014)
- Typical: Uvula retracts evenly. Soft palate rises. Gag reflex intact (Jarvis, 2014).
- Atypical: I could not find anything characteristic of MS; however, abnormal findings are as follows: absence or asymmetry of soft palate movement, deviation of uvula to side, asymmetry of tonsillar pillar movement, and hoarseness quality of sound (Jarvis, 2014).
- Cranial Nerve 11 (Spinal Accessory)
- Instructions: Shrug shoulders against resistance
- Typical: Raises shoulders with equal force (Jarvis, 2014)
- MS: Muscle weakness is possible (Jarvis, 2014)
- Cranial Nerve 12 (Hypoglossal)
- Instructions: Ask patient to stick out tongue. Ask patient to say, "light, tight, dynamite" (Jarvis, 2014)
- Typical: Tongue sticks out midline. Sound of letters are clear and distinct (Jarvis, 2014).
- MS: Articulation can be difficult in MS. Slurred speech is common (Apatoff, 2014)
(2) Balance, Coordination and Strength
How to Evaluate Muscle Strength
How to Evaluate Muscle Strength
- Check for size
- Typical: Check muscle groups and observe for bilateral symmetry (Jarvis, 2014).
- Check for strength
- Typical: Muscle strength should be equal bilaterally and should resist an opposing force (Jarvis, 2014).
- MS: Experience unequal strength (Apatoff, 2014).
- Check for tone
- Tone: Degree of tension in voluntarily relaxed muscles (Jarvis, 2014).
- Typical: During passive range of motion, should note a mild, even resistance to movement (Jarvis, 2014).
- MS: Hypotonia is possible in MS.
- Check for involuntary movements
- Typical: No involuntary movements occur (Jarvis, 2014).
- MS: Involuntary movements could occur (Apatoff, 2014).
- Gait
- Instructions: Observe a patient walk 3 to 6 m, turns and returns to the starting point.
- Typical: Person moves with a sense of freedom. Gait is smooth, rhythmic and effortless, the opposing arm swing is coordinated; the turns are smooth. (Jarvis, 2014)
- MS: Inability to tandem walk is indicative of MS. Muscle weakness makes toe and heel walking difficult. May have foot dragging (Jarvis, 2014)
- Romberg Test
- Instructions: Patient stands up with feet together and arms at side. Ask to close eyes and hold the position (Jarvis, 2014)
- Typical: Person can maintain posture and balance (Jarvis, 2014)
- MS: Loss of balance that occurs when eyes are closed. May also have an inability to stand (Jarvis, 2014)
|
|
How to Evaluate Coordination
Watch the video to the right about how to properly perform each of these coordination tests.
|
(3) Assess the Senses
MS patients typically have sensory loss (Rose, 2000). A common complaint is (hemi) paresthesia which is a sensation of tingling and pricking (needles and pins). May also have numbness (Rose, 2000).
Spinothalamic Tract
Vibration
MS patients typically have sensory loss (Rose, 2000). A common complaint is (hemi) paresthesia which is a sensation of tingling and pricking (needles and pins). May also have numbness (Rose, 2000).
Spinothalamic Tract
- Pain
- Typical: Ability to recognize pain (Jarvis, 2014)
- MS: Decrease or loss of pain, may have numbness (Rose, 2000)
- Temperature
- Typical: Ability to distinguish between hot and cold (Jarvis, 2014)
- MS: Decrease or loss of temperature
- Light Touch
- Typical: Can determine when a light touch is present (Jarvis, 2014)
- MS: Decrease or loss of sensation, may have numbness (Rose, 2000)
Vibration
- Typical: Ability to feel a vibration (Jarvis, 2014)
- MS: Severe decrease or loss of vibratory sense (Rose, 2000)
- Typical: Ability to perceive passive movement of the extremities (Jarvis, 2014)
- MS: May have reduced propioception (Rose, 2000)
- Typical: Can correctly name the object in their hand (Jarvis, 2014)
- MS: May have reduced sensation or numbness; therefore, unable to identify the object (Rose, 2000)
- Typical: Ability to “read” a number traced on their skin (Jarvis, 2014)
- MS: May have reduced sensation or numbness and unable to "read" the number (Rose, 2000)
- Typical: Ability to distinguish the separation of two simultaneous pinpoints on the skin (Jarvis, 2014)
- MS: May have reduced sensation or numbness and unable to identify the two simultaneous points (Rose, 2000)
- Typical: Able to state two simultaneous sensations (Jarvis, 2014)
- MS: May have reduced sensation or numbness and cannot state the sensations (Rose, 2000)
- Typical: Able to localize a touch sensation with their eyes closed (Jarvis, 2014)
- MS: May have reduced sensation or numbness and would not be able to localize a touch sensation (Rose, 2000)
|
(4) Testing the Reflexes
The video on the right demonstrates how to test the reflexes. Stretch Deep Tendon Reflexes
|
|
Musculoskeletal Assessment
|
RATIONALE: MS produces a lot of muscle symptoms. To determine the magnitude of how much MS affects the muscles, a MSK assessment can be done.
Test Range of Motion
|
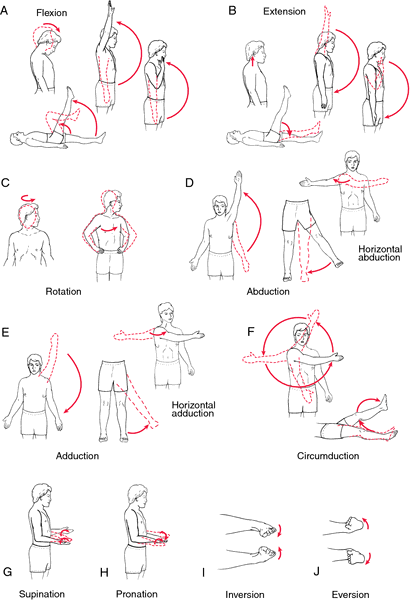
Image received from: The Free Dictionary (2016). Exercise. The Free Dictionary. Retrieved from: http://medical-dictionary.thefreedictionary.com/range+of+motion+exercise
|
